If you’re struggling with infertility and need help getting pregnant, there are fertility treatments that can help increase your chances of having a baby.
We offer many different kinds of treatment, from conventional IVF, to fertility preservation, egg and sperm donation and surrogacy.
This section describes the treatments, outlining when you might use them and what will happen if you do.
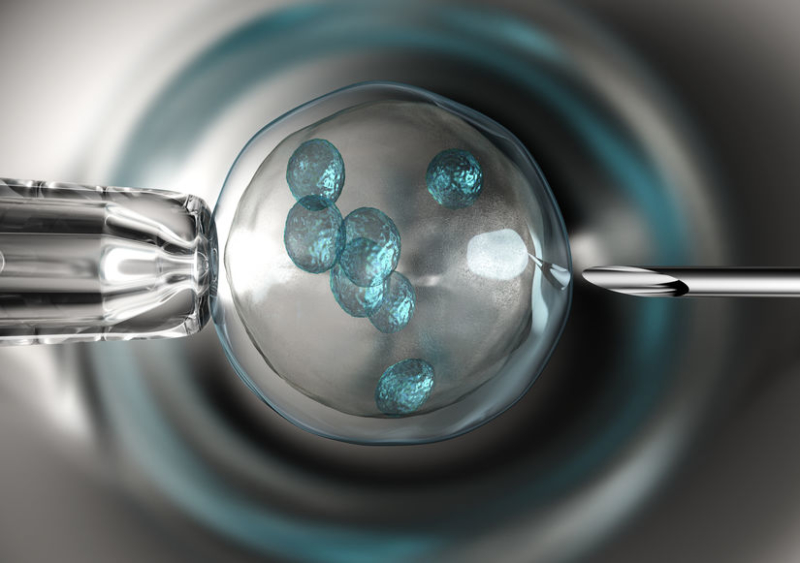
In-Vitro Fertilisation (IVF)
This involves the fertilisation of eggs with sperm in an incubator in the laboratory. IVF helps those who are struggling to conceive naturally to have the family they’ve longed for.
IVF is one of the most successful and commonly used fertility treatments.
During IVF, an egg is removed from the ovaries and fertilised by sperm in a lab. The resulting embryo is then placed back inside the womb to develop.
IVF treatment can be done using your own or donated eggs, and with sperm from your partner or donated sperm.
How does IVF work?
Every IVF treatment is different. This is because we work with you to plan a treatment that meets your specific needs and circumstances. An IVF cycle using your own fresh eggs typically follows these six steps:
1. Suppressing your natural menstrual cycle
You’ll take medication at home by injection to stop your natural hormone production and control when your eggs are released.
2. Stimulating the ovaries
You’ll take another medication for about two weeks to boost your egg production. This increases the chance of more eggs being collected.
3. Monitoring progress
You’ll have a scan to check how your eggs are doing and decide when they’ll be ready for collection. You may also have some blood tests taken.
4. Egg retrieval
A different medication is used to trigger your eggs into maturing so they can be collected from your ovaries. When your eggs are ready to be retrieved, you’ll be sedated to ensure you feel no pain or discomfort. A needle is then gently guided through the vaginal wall and used to capture your eggs, one by one. The whole process takes about 15 minutes.
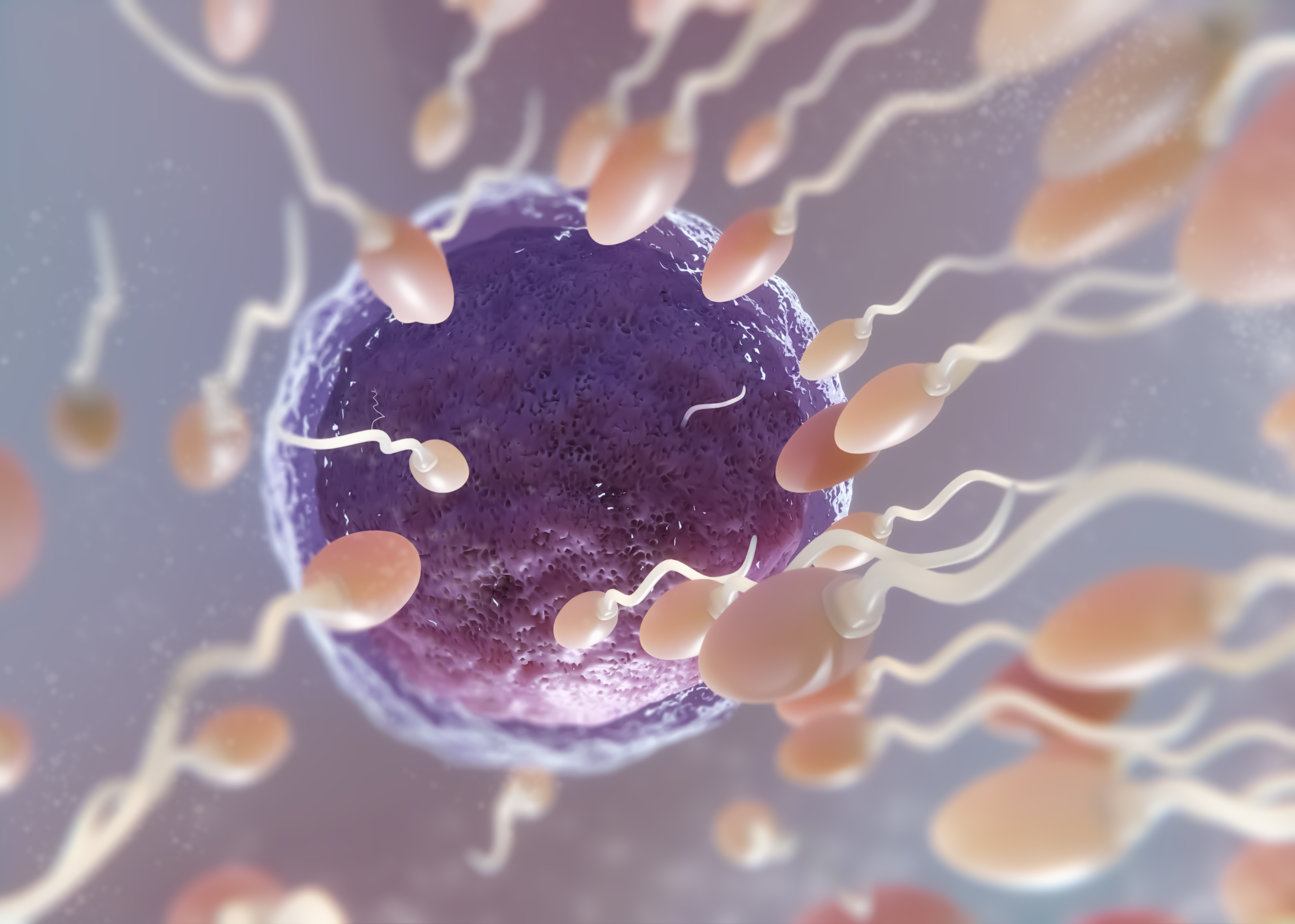
5. Fertilising the eggs
Your eggs are mixed with sperm in a laboratory to fertilise them. If necessary, each egg may be injected with a single sperm by an embryologist.
This is known as intracytoplasmic sperm injection (ICSI) and is recommended in cases where sperm count or quality is found to be lower than ideal.
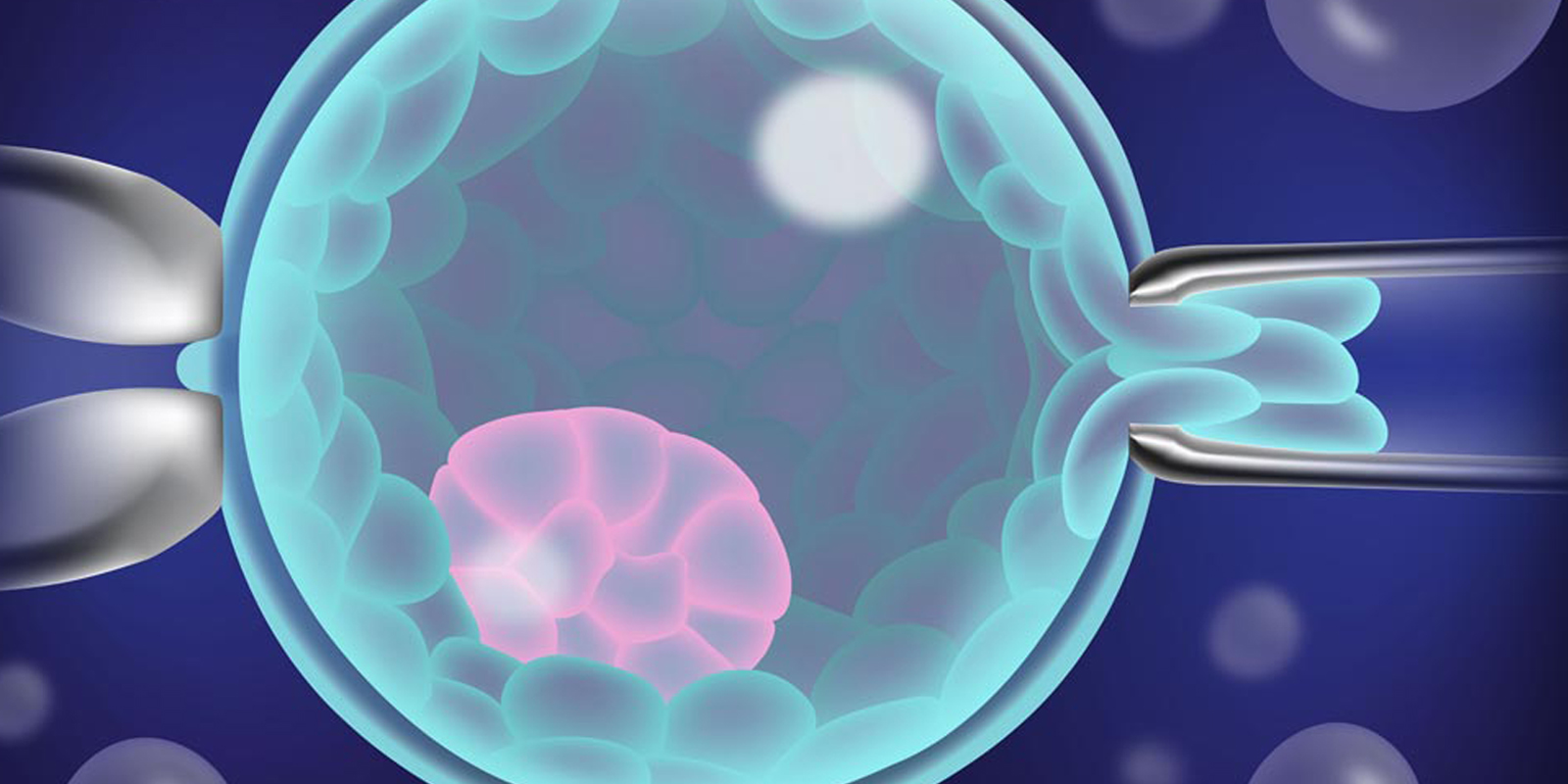
6. Embryo transfer
Your fertilised eggs, now called embryos, are incubated for up to six days.
We use a special incubator with built-in cameras, to create a time-lapse video showing embryo development. This helps us assess which embryos are strongest and most likely to implant successfully. The best one or two embryo(s) are chosen and placed into the womb to develop. Any other healthy embryos can be frozen for future use.
Who is IVF for?
IVF treatment could be a great option for you if:
- You’re a couple unable to conceive because of fertility problems
- You’ve already had IVF or another treatment, such as ovulation induction or intrauterine insemination (IUI)
- You’re a single woman using donor sperm
Whatever your situation and wherever you are in your fertility journey, we’ll work with you to develop a personalised treatment and care plan that optimises your chances of success and helps you manage the ups and downs of the experience.
Intracytoplasmic Sperm Injection (ICSI)
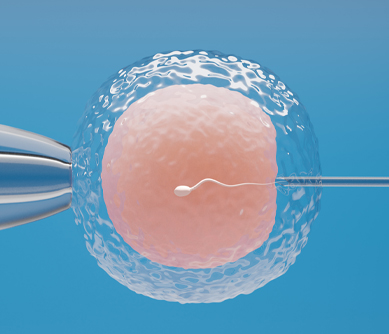
ICSI treatment involves the injection of a single sperm directly into each egg. The treatment leading up to and after ICSI is identical to the conventional IVF cycle.
For around half of couples finding it hard to get pregnant, the cause of infertility is sperm related.
ICSI is the most common and successful treatment used in this situation, performed as part of In-Vitro Fertilisation (IVF).
During a regular IVF cycle, mature eggs are removed from the ovaries, mixed with sperm in a lab, and left to fertilise. In ICSI, an embryologist injects a single sperm into each egg to fertilise it.
This removes any potential barriers to sperm getting inside an egg, maximising the chance of fertilisation.
Who can benefit from ICSI treatment?
ICSI treatment could help you if:
- You’re unable to conceive because of fertility problems
- You’ve already had IVF or another fertility treatment
When is ICSI recommended?
During your consultation, we run a series of tests to understand the cause of your fertility issues and may recommend ICSI if:
- You have a low sperm count
- Your sperm don’t move normally or are abnormally shaped
- You’re using sperm recovered via surgical sperm retrieval
- Your sperm have high levels of DNA damage
- You’ve had IVF previously and none or very few eggs fertilised
- You’re using donor eggs
- You’re using frozen eggs or sperm
Occasionally, we may recommend ICSI to you even if you have no specific sperm problems. This is because research has shown that ICSI can help improve success rates where previous rounds of IVF haven’t worked.
Frozen Embryo Transfer
A frozen embryo transfer (FET) gives you another opportunity to become pregnant without having to go through a full IVF cycle. The transfer may take place during a natural cycle or a hormone-regulated cycle.
A hormone-regulated cycle involves you taking medication to temporarily switch off your ovaries and thicken the lining of your womb. A frozen embryo transfer involving medication to regulate your hormones takes around 6–8 weeks.
A typical FET cycle includes:
- Monitoring scans
- Embryo thawing
- Post-thaw culture
- Embryo transfer
- Early pregnancy scan
Who can benefit from a frozen embryo transfer?
We offer frozen embryo transfer to couples and single women who have stored their frozen embryos with us, or those who wish to transfer their embryos to us from another clinic.
Intra Uterine Insemination (IUI)
Intrauterine insemination (IUI) is a fertility treatment where healthy, high-quality sperm are chosen from a sample in our lab and injected into your womb around the time you’re ovulating.
By introducing the sperm directly into your womb, a higher number of healthy sperm can reach the egg, increasing the chances of your egg being fertilised. IUI can be performed using your partner’s sperm or donor sperm.
Artificial insemination by partner requires a fresh sample of the partner’s sperm on the day of insemination. The semen is prepared and concentrated prior to placement in the uterus using a fine catheter (intra-uterine insemination).
We may recommend IUI treatment if:
- Your partner has a low sperm count or their sperm have poor motility, so don’t move normally.
- You’re unable to have vaginal intercourse, for example, because of a physical disability.
- You have no fertility issues, but you’d like to use donated sperm.
- You have ovulation problems.
- There’s a physical issue preventing sperm from moving up the uterine cavity, for example, a narrow cervical canal.
- You or your partner have a condition that means you need specialist help to achieve a safe pregnancy, such as men who are HIV positive having their sperm washed.
Surgical Sperm Retrieval (SSR)
This involves a simple surgical procedure to collect sperm that can then be used straight away in a fertility treatment such as ICSI, or frozen and stored for future use.
Some men have sperm being manufactured in their testes, but not present in ejaculate when the semen is analysed. The problem can be caused by a blockage, or reduced sperm production. In these cases, we can collect sperm via surgical sperm retrieval.
We use two sperm retrieval processes:
- PESA (percutaneous epididymal sperm aspiration) collects sperm directly from a long-coiled tube called the epididymis within the testicle.

- TESE (testicular sperm extraction) collects sperm from a sample of testicular tissue.
Surgical sperm retrieval may be recommended for the following reasons:
1) You have no sperm in your semen due to a blockage (obstructive azoospermia)
This may be because:
- You’ve had a vasectomy
- You’ve had an infection
- You've had a testicular injury
2) You have no sperm in your semen because of an issue with sperm production (non-obstructive azoospermia).
This may be because:
- You’ve had treatment that’s affected your fertility, such as chemotherapy or radiotherapy.
- You have a condition that affects your fertility, for example, you were born without a vas deferens, which is the tube that moves sperm away from the testicles.
- You’re producing such low numbers of sperm that they’re not reaching the vas deferens.
- You’ve had a testicle removed.
- You had surgery as a child to bring down undescended testicles.
- You’ve had a radical prostatectomy (prostate removal) due to prostate cancer.
3) You are unable to ejaculate
This may be because:
- Your semen enters your bladder instead of emerging through your penis (retrograde ejaculation).
- An issue, such as nerve damage, an injury, a condition, or a treatment, for prostate cancer for example, stops you from ejaculating when you orgasm (anejaculation).
We offer surgical sperm retrieval treatment to:
- Couples who want to use the sperm in a fertility treatment, such as ICSI
- Men who wish to preserve their sperm for use at a later stage
How long does it take to recover from surgical sperm retrieval?
Side effects are very rare following surgical sperm retrieval, but you may experience minor bruising and swelling of the scrotum.
Typically, you can return to work 24–48 hours after treatment, but strenuous activity should be avoided for 5–10 days.
We’ll prescribe you pain medication to help ease you through your recovery, and you may be given antibiotics to take before or after the procedure to help lower the risk of infection.
In-Vitro Maturation (IVM)
It involves collecting eggs from the ovaries while they are still immature. They are then grown in a laboratory for one to two days before being fertilised and replaced into the womb.
The main difference compared with IVF is that IVM doesn’t involve the use of stimulatory fertility drugs.
IVM is particularly suitable for people who prefer to avoid taking fertility drugs or who are at increased risk of complications of the drugs due to an existing medical condition, such as the one in twenty women who has polycystic ovarian syndrome (PCOS).
IVM doesn’t stimulate the ovaries at all, which means there is no risk of developing ovarian hyperstimulation syndrome (OHSS), which women with PCOS have a much greater chance of experiencing and which sometimes requires hospital admission.
However, IVM does not produce as many embryos and so currently sees lower success rates per cycle.
Every patient is unique, and we can work with you to discuss your needs and success rates, to develop the right care for you. As all treatment options ranging from mild IVF, IVM and conventional IVF are available in one place.
Freezing – Vitrification
We use a process called ‘vitrification’ to freeze sperm, eggs and embryos. It involves much more rapid cooling than other less advanced methods of freezing, and it prevents ice crystals from forming. This preserves the quality of the cells and improves the chances of success when they are thawed.
Embryo Vitrification
Embryo vitrification is now a well-established procedure. It allows us to freeze any good quality embryos that remain after embryo transfer or if transfer needs to be delayed. Embryos can be frozen at various stages, depending on how they develop. The decision to store embryos will depend on when embryo transfer takes place, and the number of good quality embryos available in the cycle. Vitrification has improved the outcomes of embryo freezing. It’s now a very reliable practice, yielding success rates as high as those achieved with fresh embryos.
Occasionally, it may be decided to vitrify all the embryos in a cycle and postpone embryo transfer. We do this to help prevent ovarian hyperstimulation syndrome (OHSS). If this is the best course of action for the individual being treated, the embryos are thawed and replaced in a subsequent cycle.
Egg Vitrification
We can use vitrification to successfully freeze eggs immediately after the collection procedure. This is important for women who would like to store eggs before undergoing chemo- or radiotherapy, or other treatments that might affect their fertility in the future.
We also store eggs for women who are not ready to start a family now, but who recognise the importance of storing eggs while they are younger. Eggs collected and stored earlier in life are of a better quality than those women produce later on. Patients who choose to freeze eggs when they are under 35 tend to have higher success rates.
Sperm Freezing
You may need to store sperm for fertility preservation before certain medical procedures or in the course of a fertility treatment cycle:
- Prior to chemo or radiotherapy
- Prior to vasectomy
- Prior to any surgery that may result in impaired fertility
- Prior to a fertility treatment cycle and after sperm has been retrieved via surgery
- Prior to a fertility treatment cycle as a ‘back-up’ sample for the day of treatment